
Tears are not the same from the outer layer to where it touches the cornea, there are three indistinct layers which are mucus layer, aqueous layer and lipid or oily layer.
The tear layers
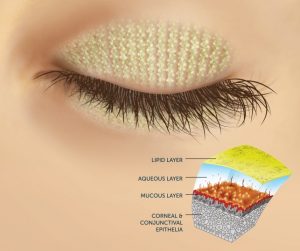
- The Lipid or oily layer: This is the outermost layer of tear film formed at air-tear interface from the
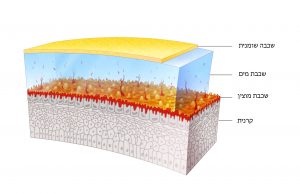 secretions of mainly the meibomian glands (see above). This layer prevents the tear from evaporating too quickly.
secretions of mainly the meibomian glands (see above). This layer prevents the tear from evaporating too quickly. - The Aqueous layer: The bulk of tear film is formed by this intermediate layer which consists of tears secreted by the lacrimal gland (see above). This layer mainly comprises of water and small quantities of solutes such as sodium chloride, sugar, urea and proteins. Therefore, it is salty in taste. It also contains antibacterial substances.
- The Mucus layer: It is the innermost and thinnest layer of the tear film. It consists of mucin secreted by conjunctival goblet cells and glands of Manz. It converts the corneal surface to hydrophilic one (watery). This layer allows the even distribution of the tears on the cornea and the protection of all the corneal surface by the tear film.
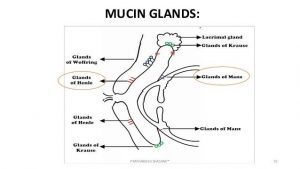
The lacrimal system
sits on the outer upper part of your eye, each eye has its own. It consists of:
- The lacrimal gland, which secretes your tears, and its excretory ducts, which convey the fluid to the surface of your eye;
- The lacrimal canaliculi, the tear sac, and the tear duct, by which the fluid is conveyed into the cavity of your nose. After the tears have washed your eyes they are drained to your nose, so that we are not tearing all day!

- The Meibomian glands are located at the rim of the eyelids. There are approximately 50 glands on your upper eyelids and 25 glands on your lower eyelids. They are responsible for the production of meibum, an oily substance that prevents evaporation of your tears. Meibum prevents tear spillage onto the cheek and makes the closed lids airtight.
What is the Dry Eye Disease exactly? And why does the disease develop?
Dry eye syndrome Pathophysiology
Lately there’s been a lot of research and development in the field of the Dry Eye Syndrome.
The latest and most updated scientific data is summarized and explained in the following paragraphs. Your Dry Eye Symptoms will be classified according to the committee of the National Eye Institute new classification system for the various types of dry eye syndrome. [Lemp MA Report of the National Eye Institute/Industry Workshop on clinical trials in dry eyes. CLAO J.1995;21221- 232 ]
There are 2 main categories of Dry Eye: Aqueous tear production deficient and evaporative dry eye.
1. Evaporative Dry Eye Disease: This is the more common type and is mostly caused by Meibomian gland dysfunction. [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3772773/]
- The Meibomian gla
 nds are oil producing glands in the lid margins of both your upper and lower eyelids. These glands produce the oil which comprises the outermost layer of your tears. Whenever the eye blinks, they produce oil coating the tear layer, protecting it from evaporation too quickly. When these oils are reduced, the evaporation of your tears from the surface of your eyes is increased and your eyes become dry quickly. This is the common cause for dry eye when you are working on your computer screen, using your cell phone, reading on a tablet, document,
nds are oil producing glands in the lid margins of both your upper and lower eyelids. These glands produce the oil which comprises the outermost layer of your tears. Whenever the eye blinks, they produce oil coating the tear layer, protecting it from evaporation too quickly. When these oils are reduced, the evaporation of your tears from the surface of your eyes is increased and your eyes become dry quickly. This is the common cause for dry eye when you are working on your computer screen, using your cell phone, reading on a tablet, document, - watching T.V., driving, etc.
- Meibomian Gland Dysfunction (MGD) is a chronic, diffuse abnormality of the Meibomian glands.
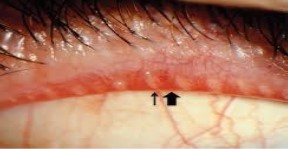 It is very common in the young and older population. It is related to blepharitis, Meibomitis, and/ or ocular rosacea.
It is very common in the young and older population. It is related to blepharitis, Meibomitis, and/ or ocular rosacea. - Blepharitis is an inflammation of the eyelids, involving the part of the eyelid where the eyelashes grow. It is usually bilateral but can be felt more in one eye than the other. It is Chronic and can be unnoticed for years, thus causing anatomic destruction of the structures of the eyelid. Up to 47% of general population suffers from Blepharitis. It is also called in popular language “inflammation or infection of the eyelid, or red eyelids”. Dry eye is the complication of Blepharitis.
- Like other surfaces of our body as the skin and the mouth, our eyelids also have bacteria spread over them. A healthy biofilm allows the eye to be wet and see well. However, some bacteria in the biofilm, like Staphylococcus are pathological, produce toxins,and cause inflammation. When there is Meibomian Gland Dysfunction, the biofilm is unbalanced and there is excessive production of toxins which irritates the eyelid and deteriorates the quality of the tears. Those toxins may be the most important cause of MGD. Blepharitis may appear in children as well as the elderly, and depending on the specific kind of toxin that the germs that you were born with produce.
- Meibomitis, is an inflammation of the meibomian glands where the oils produced are too thick and they don’t flow out of the gland openings. The meibum becomes stagnant and bacteria starts feeding on the thickened stagnant meibum. Bacteria reproduces and secretes toxins that cause the lids to become red and inflamed.
- Ocular rosacea is an ocular manifestation of a skin condition known as rosacea. It is an inflammation that affects the eyelids as well as the cornea. While the exact cause is unknown, the condition may be associated with environmental factors such as massive sun exposure, stress or specific medications. Symptoms of ocular rosacea are very similar to those of dry eye, it is a more severe condition than the common blepharitis, your doctor will know the difference and will adapt the appropriate treatment.
2. Aqueous tear production deficient: This category includes Sjögren-associated dry eye syndrome and non-Sjögren associated dry eye syndrome.
- Sjogren Syndrome is an autoimmune disease which may be primary or secondary (due to another autoimmune disease like Lupus), often characterized with dry mouth in addition to dry eye. Sjogren is positively diagnosed by taking a blood test and a biopsy. It is a rare and serious disease and it requires treatment of the underlying disease in parallel to the eye care. [https://jamanetwork.com/journals/jamaophthalmology/fullarticle/269914]
- Non- Sjogren dry eye is a group of local and systemic disorders giving rise to deficiency of tear components or their distribution. Any deficiency of the major components of the tears may cause this syndrome:
- Aqueous deficiency due to lacrimal gland failure
- Mucin deficiency due to Goblet cell deficiency (Mucin is the major source of tear viscosity, hence it is the basis for its lubricative function) [https://link.springer.com/chapter/10.1007/978-1-4615-2417-5_81]